A groundbreaking clinical study, spearheaded by Stanford Medicine and an international consortium of researchers, has unveiled a revolutionary tiny wireless chip implanted at the back of the eye, which, when paired with advanced smart glasses, has demonstrably restored partial vision for individuals suffering from an advanced and previously untreatable form of age-related macular degeneration (AMD). The pioneering trial, published with significant fanfare in the esteemed New England Journal of Medicine on October 20th, reported that a remarkable 27 out of 32 participants regained the crucial ability to read within a year of receiving the innovative implant, marking a pivotal moment in the quest to restore functional vision.
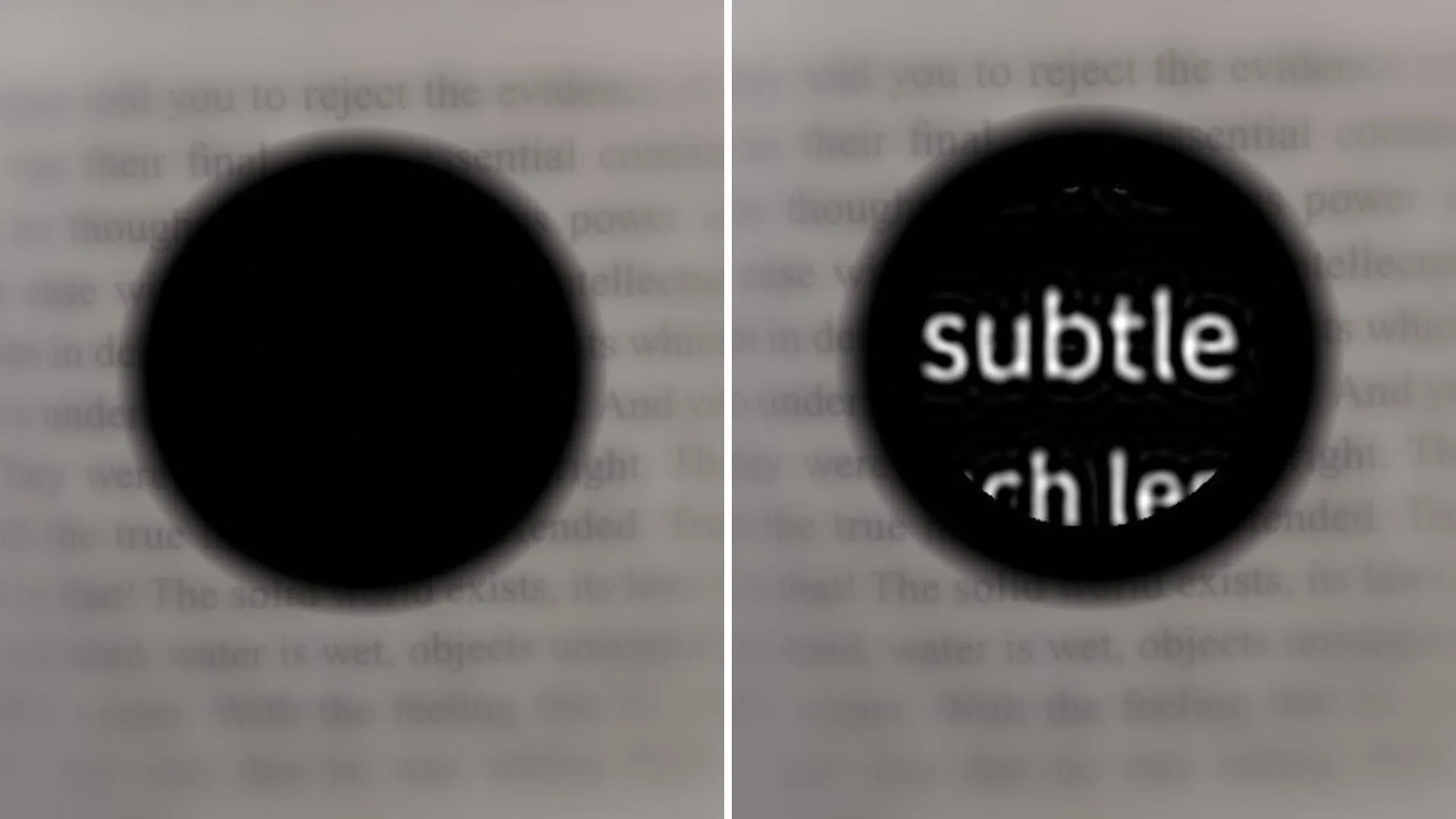
This significant achievement is attributed to the PRIMA system, an ingenious prosthetic eye device developed at Stanford Medicine, which represents the first of its kind to offer usable vision to patients facing otherwise irreversible vision loss. The technology’s remarkable capability lies in its ability to enable patients to discern shapes and patterns, a level of visual perception termed "form vision." This contrasts sharply with prior prosthetic devices, which, as noted by Daniel Palanker, PhD, a professor of ophthalmology and co-senior author of the study, primarily offered only light sensitivity rather than true form vision. "We are the first to provide form vision," Palanker stated, underscoring the profound nature of this advancement. The collaborative research effort was co-led by José-Alain Sahel, MD, a professor of ophthalmology at the University of Pittsburgh School of Medicine, with Frank Holz, MD, of the University of Bonn in Germany, serving as the lead author, highlighting the global reach and collective expertise driving this transformative technology.
The PRIMA system operates through a sophisticated interplay of two key components: a miniature camera integrated into a pair of specialized smart glasses, and a wireless microchip surgically implanted within the retina. The external camera captures visual information from the patient’s surroundings and transmits it via infrared light to the retinal implant. This implant then meticulously converts the infrared signals into electrical impulses. These artificial electrical signals effectively bypass and substitute for the damaged photoreceptor cells, the natural light-detecting cells in the retina that are essential for transmitting visual data to the brain. This ingenious mechanism allows the surviving retinal neurons, which process visual information, to interpret these signals and reconstruct a semblance of sight.
The development of the PRIMA project is not an overnight success but rather the culmination of decades of dedicated scientific endeavor, encompassing numerous iterations of prototypes, extensive animal testing, and an initial human trial. Dr. Palanker’s initial conception of this revolutionary approach dates back two decades, sparked during his work with ophthalmic lasers for treating eye conditions. He observed the eye’s inherent transparency and recognized the potential to deliver visual information directly through light. "The device we imagined in 2005 now works in patients remarkably well," he remarked, reflecting on the long journey from concept to clinical reality.
The recent trial specifically focused on participants suffering from geographic atrophy, an advanced stage of age-related macular degeneration. This debilitating condition progressively erodes central vision and affects over 5 million people worldwide, standing as the primary cause of irreversible blindness in older adults. In AMD, the crucial light-sensitive photoreceptor cells in the macula, the central part of the retina responsible for sharp, detailed vision, deteriorate. This leaves individuals with only limited peripheral vision. However, a critical factor for the PRIMA system’s success is that many of the retinal neurons responsible for processing visual information often remain intact even as photoreceptors are lost. PRIMA ingeniously capitalizes on these surviving neural structures.
The implant itself is remarkably small, measuring a mere 2 by 2 millimeters, and is precisely placed in the retinal area where photoreceptors have been lost. A key distinction of the PRIMA chip is its response to infrared light, emitted by the smart glasses, rather than visible light that natural photoreceptors detect. "The projection is done by infrared because we want to make sure it’s invisible to the remaining photoreceptors outside the implant," explained Dr. Palanker. This design choice is crucial for ensuring that the prosthetic vision does not interfere with the patient’s existing, albeit limited, peripheral vision.
This strategic design fosters a synergistic integration of natural and artificial vision. Patients are able to simultaneously utilize their existing peripheral vision and the newly restored central prosthetic vision, significantly enhancing their ability to navigate their environment and orient themselves. "The fact that they see simultaneously prosthetic and peripheral vision is important because they can merge and use vision to its fullest," Dr. Palanker emphasized. Furthermore, the PRIMA implant is photovoltaic, meaning it generates its own electrical current solely from light. This intrinsic power source allows it to operate wirelessly and be safely positioned beneath the retina, eliminating the need for external power sources or invasive cables that characterized earlier generations of artificial eye devices.
The impact of the PRIMA system on participants’ daily lives has been profound, particularly in their ability to engage in activities previously thought impossible. The trial involved 38 patients aged 60 and above, all diagnosed with geographic atrophy due to AMD and possessing vision worse than 20/320 in at least one eye. Following implantation of the chip in one eye, and a period of four to five weeks of adaptation, patients began using the smart glasses. While some individuals could discern patterns immediately, all participants demonstrated significant improvement in visual acuity over several months of dedicated training. Dr. Palanker drew a parallel to cochlear implants, noting that "It may take several months of training to reach top performance — which is similar to what cochlear implants require to master prosthetic hearing."
The results of the one-year trial were overwhelmingly positive. Of the 32 patients who completed the study, a significant majority, 27, were able to read. Moreover, 26 participants exhibited clinically meaningful improvement in visual acuity, defined as the ability to read at least two additional lines on a standard eye chart. On average, participants experienced an improvement of five lines on the eye chart, with one individual achieving an astonishing twelve-line improvement. The prosthesis proved invaluable in everyday tasks, enabling participants to read books, decipher food labels, and recognize subway signs. The adjustable features of the smart glasses, including contrast and brightness controls and up to 12x magnification, further enhanced their functional vision. This positive impact translated into user satisfaction, with two-thirds of participants reporting medium to high levels of contentment with the device. While nineteen participants experienced side effects, such as ocular hypertension, peripheral retinal tears, and subretinal hemorrhage, these were generally not life-threatening and resolved within two months.
Looking towards the future, the PRIMA device, currently providing black-and-white vision, is poised for further enhancement. Dr. Palanker is actively developing software to introduce a full range of grayscale, a critical step for applications like face recognition, which he identified as a high priority for patients alongside reading. "Number one on the patients’ wish list is reading, but number two, very close behind, is face recognition. And face recognition requires grayscale," he explained.
Beyond grayscale capabilities, research is underway to engineer chips with significantly higher resolution. The current resolution is limited by the pixel size on the chip; the existing chips feature 378 pixels, each 100 microns wide. The next generation of chips, already showing promise in rat trials, aims for pixels as small as 20 microns wide, potentially housing 10,000 pixels. This advancement could elevate a patient’s vision to 20/80, with the added benefit of electronic zoom potentially bringing them close to 20/20 vision. Dr. Palanker also intends to explore the applicability of the PRIMA device for other forms of blindness caused by photoreceptor loss. "This is the first version of the chip, and resolution is relatively low," he stated, optimistic about the future. "The next generation of the chip, with smaller pixels, will have better resolution and be paired with sleeker-looking glasses."
The groundbreaking study benefited from the expertise and contributions of a vast network of researchers from institutions worldwide, including the University of Bonn, Germany; Hôpital Fondation A. de Rothschild, France; Moorfields Eye Hospital and University College London; Ludwigshafen Academic Teaching Hospital; University of Rome Tor Vergata; Medical Center Schleswig-Holstein, University of Lübeck; L’Hôpital Universitaire de la Croix-Rousse and Université Claude Bernard Lyon 1; Azienda Ospedaliera San Giovanni Addolorata; Centre Monticelli Paradis and L’Université d’Aix-Marseille; Intercommunal Hospital of Créteil and Henri Mondor Hospital; Knappschaft Hospital Saar; Nantes University; University Eye Hospital Tübingen; University of Münster Medical Center; Bordeaux University Hospital; Hôpital National des 15-20; Erasmus University Medical Center; University of Ulm; Science Corp.; University of California, San Francisco; University of Washington; University of Pittsburgh School of Medicine; and Sorbonne Université. Funding for this transformative research was generously provided by Science Corp., the National Institute for Health and Care Research, Moorfields Eye Hospital National Health Service Foundation Trust, and University College London Institute of Ophthalmology, underscoring the collaborative and well-supported nature of this significant scientific endeavor.